|Videos|April 2, 2022
Educated Patient® Multiple Myeloma Summit Newly Diagnosed Myeloma Presentation: March 12, 2022
Author(s)Darlene Dobkowski, MA
Watch Dr. Krina K. Patel, an associate professor and center medical director for the Department of Lymphoma-Myeloma at The University of Texas MD Anderson Cancer Center discuss treatment for newly diagnosed myeloma.
Advertisement








Although most patients with multiple myeloma cannot be cured of their disease at the present time, an expert emphasizes the importance of using the best therapies when a patient is newly diagnosed in an attempt to destroy as many myeloma cells as possible and to potentially improve quality and quantity of life.
“Now, we have lots of new therapies down the road, but really having the best response at the beginning sets that pace to make sure that we give you the best shot later down the road,” said Dr. Krina K. Patel, an associate professor and center medical director for the Department of Lymphoma-Myeloma at The University of Texas MD Anderson Cancer Center in Houston, in an interview with CURE®.
Patel discussed frontline treatment options in patients newly diagnosed with multiple myeloma during the CURE® Educated Patient® Multiple Myeloma Summit.
Navigating Treatment Options
With the vast availability of
Patel said that with the different regimens available to treat patients with newly diagnosed multiple myeloma, she believes the best regimen available may be the one assessed in the GRIFFIN trial: Darzalex (daratumumab), which is an immune therapy, specifically a monoclonal antibody; Revlimid (lenalidomide), an immunomodulatory drug; Velcade (bortezomib), a proteasome inhibitor; and dexamethasone, a steroid.
“That group of four drugs has shown that patients can get into that really deep response over time,” Patel said. “These patients on the (GRIFFIN) trial actually got those four cycles, which is 21 days each, and then went into stem cell transplants, so these are transplant-eligible patients, and then had more maintenance (therapy) of either (Darzalex/Revlimid) or (Revlimid alone).”
Patel added that the jury is still out on whether adding Darzalex to Revlimid for maintenance therapy after a stem cell transplant is the right approach for all patients. She believed that most oncologists would use Revlimid maintenance for standard-risk patients.
For high-risk patients, Patel said that a quadruplet therapy is still a great option, but another option may be Kyprolis (carfilzomib), a proteasome inhibitor, plus Revlimid and dexamethasone. There have been several studies conducted assessing the benefit of that triplet therapy plus transplant. One concern about this approach is the increased risk for heart-related side effects.
Patel said
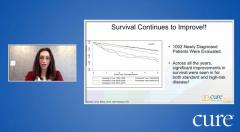
“(Researchers) just showed us the five-year overall survival rates (from the MAIA trial) that are so high,” Patel said. “Patients over time are doing better and better with their myeloma being controlled longer and longer. Now we’re looking at ways to maybe take off some of the medications over time to say, can we go to maintenance a little bit earlier? Again, the biggest things to look at are, we want to get to that best response, and then we also want to decrease toxicity.”
Assessing Treatment Effectiveness
More research is also being conducted looking at
“That’s where some of these new upfront therapies are looking at to get more patients into that deeper response, that we can’t find those myeloma cells with the best technology we have right now,” Patel explained. “We know that, that leads to a better progression-free survival so that myeloma stays hibernating for a lot longer.”
A study published in the Journal of Clinical Oncology in 2021 reviewed the effectiveness of minimal residual disease-negative assessments in patients treated with Darzalex, Kyprolis, Revlimid and dexamethasone, “which is sort of all of our best drugs at the front,” Patel said. Findings from the study demonstrated that high rates of minimal residual disease-negativity occurred with this treatment approach.
“If we can show that if you get to (minimal residual disease) negativity, which we can do that in the first six months or a year of a study, and then prove that, that actually tells us that those patients are going to do well, then I think that’d be a great surrogate marker for the (Food and Drug Administration) to use to hopefully in the future help us approach trials earlier instead of taking years and years,” Patel explained.
Even with the advancements that have been made in the treatment of patients with newly diagnosed multiple myeloma, there are even more in the pipeline that patients can anticipate in the next few years.
“I joke with my patients all the time that if you came to me six months ago, we would have been doing this (treatment) differently,” Patel said.
For example, immunotherapy, which is currently used in patients with relapsed/refractory multiple myeloma, is being assessed in earlier lines of therapy and newly diagnosed patients.
“We’ve exponentially grown in terms of how to manipulate the immune system to help us fight the myeloma, and even the antigens that it goes after, so not just the mechanism of action of these drugs, but how it is going to approach the myeloma,” Patel explained.
A Team-Approach to Care
As more treatments for newly diagnosed multiple myeloma become available, Patel emphasized the importance of seeing a specialist to make sure all treatment decisions are appropriate, even if that means seeking a second opinion.
“It’s supposed to be a team approach to make sure we get the best outcomes to all patients,” Patel said. “But really, having that specialist in the background (in addition to a community oncologist) that can help make sure that you’re getting the most up-to-date treatment and making sure you need treatment.”
Having an extra set of eyes on your treatment options and on you as a patient can also be helpful when it comes to supportive medications, which can be used to counteract some of the effects of multiple myeloma treatments.
“We want to make sure you're on blood thinners when you're on lenalidomide (Revlimid) so you don't get clots,” Patel explained. “We want to make sure you're on bone-strengthening medicines because that actually helps keep the myeloma away and helps build your bones back if you have bone disease. We want to make sure you're on the right antiviral medicines so you don't get shingles because all (of) these medicines can cause them. I think for all those different reasons, having that extra look at your case and helping you along the way. Your doctor is going to be your doctor who treats and takes care of everything. But we're there to make sure there's not something missing or we need to change therapy if it's not working correctly.”
For more news on cancer updates, research and education, don’t forget to
Advertisement
Related Content
Advertisement





Advertisement
Advertisement
Trending on CURE
1
Balance Exercises for Patients With Cancer: How the Single-Leg Stand Builds Stability
2
Clock Touches: An Advanced Balance Exercise for Patients with Cancer
3
Wildfire Smoke and Cancer Risk: What Patients Should Know
4
Family History of Cancer Fuels Oncology Nurse's Passion for Patient Care
5